A ticking time bomb in your tooth called amalgam
Seeing that “silver filling” as nothing more than something old and ugly is to underestimate what may be happening beneath the surface. In many cases, what looks like just an old filling is actually hiding serious structural cracks in the tooth – true lines of fragility that slowly form over the years until, suddenly, the tooth breaks.
That’s why I often say, in the office, that some dental amalgam restorations work like a “ticking time bomb”: they stay silent for a long time, but have already left the tooth vulnerable to an unexpected fracture. And when the tooth does break, the damage is often so great that it requires root canal treatment, extensive crowns or even extraction.
Understanding why this happens, when amalgam is a risk and how modern dentistry can intervene safely is essential to protect your tooth structure before the problem appears.
What is dental amalgam and why was it used so much?
Dental amalgam is a metallic restorative material that has been used in dentistry for more than 150 years. It is made of an alloy of metals (such as silver, copper and tin) mixed with metallic mercury, which reacts and hardens, forming a strong and durable restoration. On average, amalgam contains around 50% mercury by weight, chemically bound to the metal alloy.
For decades, it was the main choice for restoring posterior teeth because it is:
- Durable in environments with high chewing loads
- Relatively inexpensive
- Technically predictable in many clinical situations
Major international organizations, such as the American Dental Association (ADA) and the International Association for Dental Research (IADR), emphasize that, for the general population, dental amalgam is considered a safe and effective restorative material when properly indicated.
On the other hand, the world is moving toward a progressive reduction in the use of amalgam, mainly for environmental reasons (due to the mercury component), and not because existing restorations have been declared “toxic” for everyone. The Minamata Convention – an international treaty on mercury – sets out measures to reduce and, in many countries, gradually eliminate the use of amalgam in the coming decades.
Simply put: the material was important in the history of dentistry, it is still considered safe in many contexts, but it is no longer the protagonist in an approach that seeks to preserve tooth structure as much as possible and reduce environmental impacts.
How dental amalgam can compromise tooth structure
Even though it is resistant, dental amalgam has physical characteristics that can, over time, affect the integrity of the tooth that holds it – especially in large restorations that involve several surfaces of the tooth.
Some important points:
- Amalgam does not bond chemically to the tooth; it is retained by mechanical retention, which often requires removing more healthy tooth structure to “lock” the material in place.
- It is a rigid material, with a pattern of expansion and contraction in response to temperature changes (hot and cold drinks, etc.) that is different from natural tooth tissue.
- This volumetric “back and forth” over the years generates internal stress in the tooth walls, especially in the cusps (the highest parts of the tooth) and in already weakened regions.
Studies evaluating teeth restored with amalgam show that, in molars with extensive restorations, there is greater cusp flexure and higher stress levels in tooth structure compared with intact teeth, which favors the appearance of cracks over time.
In clinical practice, this means: the tooth may look intact, but the rigid metal restoration is slowly acting like a wedge, forcing the tooth from the inside out.
Silent cracks: when the tooth looks strong but is vulnerable
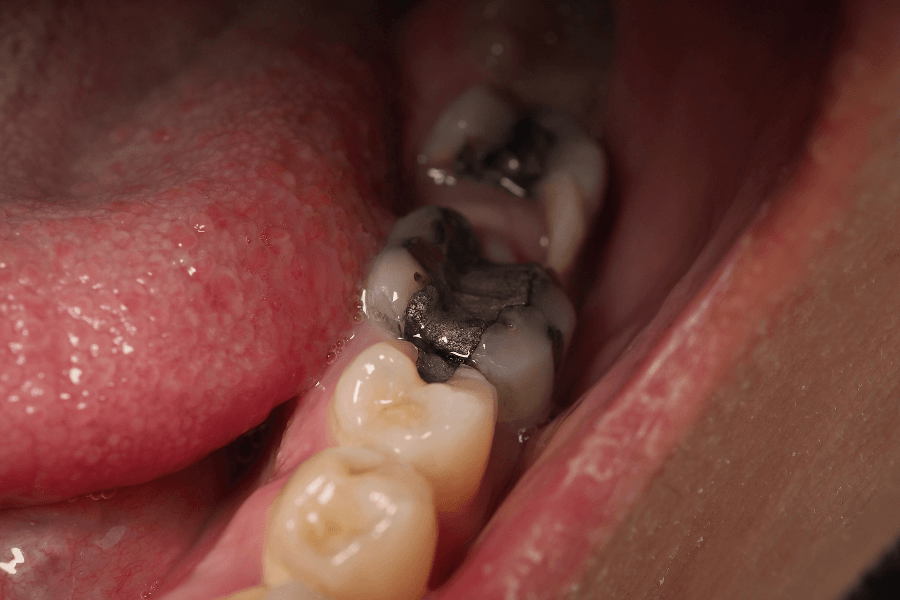
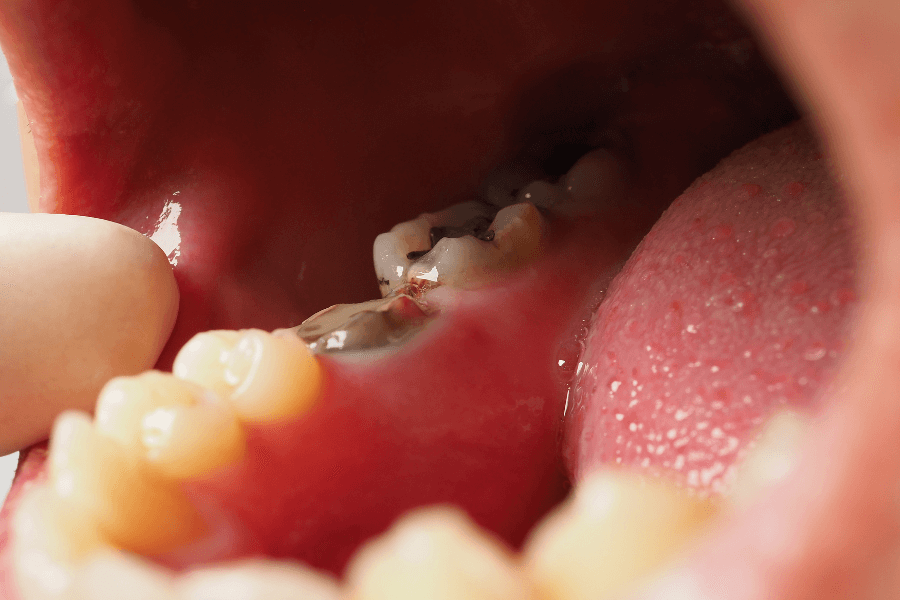
In the clinical image I often show patients, we see an old dental amalgam restoration surrounded by very fine, almost transparent lines in the tooth structure. These lines are not just superficial marks: they are structural cracks.
These microfractures:
- Are often invisible to the naked eye without proper magnification
- May cause no pain for years
- Can be identified in a detailed clinical examination with good lighting, magnification, dyes and radiographs
- Increase the risk of a sudden fracture, often during a trivial moment (like biting something slightly harder)
In some cases, the fracture is superficial and allows for conservative restoration. In others, the fracture line goes deeper toward the root. When that happens, the tooth may:
- Require root canal treatment and rehabilitation with a crown, or
- Become non-restorable, leading to extraction
This is where the idea of a “ticking time bomb” comes in: the tooth does not warn you, it does not hurt, but structurally it is already compromised.
Not every dental amalgam is a problem, but every case needs to be evaluated
It is important to make a responsible distinction: it is not correct to say that every amalgam restoration will necessarily cause fractures or that it must be replaced just because it exists. Recent studies analyzing the relationship between tooth fractures and the presence of amalgam restorations have not found, under certain conditions, a statistically significant difference in fracture risk solely because the tooth has amalgam.
So, what is the key point?
- Very extensive restorations, involving several cusps, increase the chance that the tooth becomes weakened, whether with amalgam or other materials;
- In already cracked teeth, with symptoms such as pain on chewing, localized sensitivity or a history of fractures, rigid metal restorations can worsen the situation;
- Old restorations that are infiltrated or show signs of corrosion and defective margins deserve extra attention.
Therefore, the decision to replace or keep a dental amalgam restoration must be based on:
- Careful clinical examination;
- Radiographic analysis;
- Assessment of the size and extension of the restoration;
- Presence (or absence) of cracks and symptoms;
- The patient’s overall health context and expectations.
Replacing amalgam “because it’s trendy,” without a real clinical indication, is also a risk: every time we intervene in a tooth, we remove a bit more structure. The balance lies in knowing when amalgam is protected and stable – and when it has, in fact, become a point of fragility.
How modern dentistry safely replaces amalgam
When we identify that a dental amalgam restoration is bringing structural risk to the tooth (cracks, leakage, loss of support, symptoms), the plan for replacement must be made carefully.
Some important steps:
1. Isolation and safety
The ideal approach is to work with proper isolation (such as rubber dam), careful removal technique in chunks whenever possible, and responsible disposal of the material, in accordance with environmental and biosafety regulations.
2. Assessment of remaining tooth structure
After removing the amalgam, we evaluate how much healthy structure is left. In many cases, we realize that the amount of remaining dentin and enamel is smaller than it seemed when looking at the finished restoration.
3. Choosing the type of rehabilitation
According to the case, we may indicate:
- Adhesive composite resin restorations, when the loss of structure is moderate;
- Ceramic onlays or overlays (indirect restorations that cover and reinforce weakened cusps);
- Crowns, in cases where the remaining structure is very reduced.
Modern adhesive materials make it possible to bond the restoration to the tooth, helping to redistribute forces and reduce the risk of new cracks when properly planned.
4. Control of parafunctions, such as bruxism
In patients who clench or grind their teeth, it is often necessary to complement the treatment with a night guard (occlusal splint) and occlusal adjustment to protect the restored tooth.
The goal is not simply to “swap silver for white,” but to rebuild the tooth in a more biomimetic way, respecting its anatomy, function and limits.
Frequently asked questions about dental amalgam
“Is amalgam poison? Is it poisoning me?”
The main international scientific organizations indicate that, for the general population, dental amalgam is considered a safe and effective material when properly indicated. The mercury present is chemically bound to the metal alloy, and exposure levels in patients with restorations within normal standards are considered below risk limits for healthy individuals.
There are specific groups – such as people with a known allergy to amalgam components or with severe kidney disease – who may require a different approach. That’s why individual assessment is essential.
“Do I need to remove all the amalgam fillings from my mouth?”
There is no universal recommendation to remove all dental amalgam restorations just because they exist. Unnecessary replacements can weaken teeth that are currently stable and crack-free, and expose the patient to complex procedures without real benefit.
The focus should be on:
- Identifying restorations that are already compromising tooth structure;
- Planning replacement in a safe and gradual way if multiple teeth are involved;
- Prioritizing teeth with cracks, leakage or symptoms.
“Are resin and ceramic always better?”
Modern aesthetic materials, such as composite resins and ceramics, offer important advantages: bonding to the tooth, the possibility of more conservative preparations and excellent esthetic results. However, every material has its limitations and technical requirements.
In many situations, with good planning, these materials allow a more conservative and functional rehabilitation than maintaining an old, cracked dental amalgam. In other cases, the best decision may be to monitor a stable restoration with no signs of risk.
The central point is: the choice of material must be personalized, and not based solely on color or esthetic preference.
Schedule your evaluation and find out if your dental amalgam is a ticking time bomb
If you look in the mirror and still see “silver fillings,” that doesn’t automatically mean your teeth are in danger – but it is a clear sign that it’s worth getting them checked. Many cracks are silent and only show up in detailed examinations, with a trained eye and appropriate diagnostic resources.
At Clínica Debora Ayala, each tooth with dental amalgam is analyzed considering:
- The integrity of the surrounding structure;
- The presence of cracks and leakage;
- Your history of symptoms, pain or fractures;
- Your general health context and long-term goals.
The goal is not to create fear, but to offer qualified information so that you can make conscious decisions: when to keep, when to monitor and when to replace an old restoration before it turns into an unexpected fracture.
Contact the Debora Ayala Clinic team and schedule a personalized appointment. Let’s assess together whether your amalgam is just a reminder of an older era in dentistry or whether it has already become a ticking time bomb that needs to be safely defused.
Dr. Debora Ayala – CRO 41.974/SP
Read Also
