
Pain at the back of the mouth may be a sign of a wisdom tooth: Why the right timing of evaluation changes treatment
Wisdom tooth pain often starts subtly. Sometimes it appears as mild discomfort at the back of the mouth, sensitivity while chewing, discomfort that comes and goes, or the feeling that something is “pressing” in the posterior region. Because it seems like a minor symptom, many patients delay evaluation. The problem is that when a third molar begins to show signs, we are not always dealing with something simple or temporary. In many cases, the pain is only the first warning of a process already underway, such as gum inflammation around the tooth, lack of space for eruption, pressure on the second molar, or close contact with important anatomical structures.
That is exactly why, at Clínica Debora Ayala, the topic of wisdom teeth is not treated simply as “extract or not extract.” The central point is understanding when to intervene, how to intervene, and what the most favorable biological timing is for each case. Clinical literature and documents from the American Association of Oral and Maxillofacial Surgeons reinforce that third molar management must consider signs of disease, risk of progression, age, root development, relationship with the inferior alveolar nerve, and the possibility of safe follow-up when there is no immediate indication for removal.
Not all pain at the back of the mouth is the same
When a patient reports wisdom tooth pain, the first step is not to automatically assume that extraction will be necessary. This pain can have different origins. In some cases, it is related to pericoronitis, which is inflammation of the tissues around a partially erupted third molar. In others, there may be mechanical pressure, chronic gingival inflammation, decay in the wisdom tooth or the neighboring tooth, root resorption of the second molar, or biofilm accumulation in an area that is difficult to clean. Recent clinical guidelines on the diagnosis and indication for third molar extraction emphasize exactly this need to differentiate between conditions before deciding on treatment.
This distinction matters because the same sensation of “discomfort at the back of the mouth” may represent very different stages of a problem. In one patient, it may simply be a tooth under observation. In another, there may already be recurrent inflammation, periodontal damage to the second molar, or increased surgical risk due to the stage of root development and proximity to the nerve. That is why excellent care does not begin with the procedure; it begins with an accurate reading of the case.

What does it mean for a wisdom tooth to be impacted?
A wisdom tooth, or third molar, is considered impacted when it cannot erupt properly into the mouth because of lack of space, inadequate position, or bony and gingival barriers. A 2026 consensus on third molar health reinforces that impacted third molars increase the risk of periodontitis, decay, and root resorption in the adjacent tooth, especially when they remain partially or completely impacted for long periods.
In practice, this helps explain why a wisdom tooth often creates problems “silently” before causing intense pain. A patient may go months or years with a poorly positioned third molar without alarming symptoms, while the condition progresses slowly. When the pain finally becomes strong enough to motivate consultation, the inflammation is usually more established, the roots more developed, and the surgery potentially more demanding.
Why timing of intervention matters so much
One of the most important aspects in wisdom tooth management is timing. The summary you provided is essentially correct: the moment of intervention influences the degree of surgical complexity and treatment predictability. Although the decision to extract should not be automatic or based solely on age, the literature shows that extractions performed in younger patients, before greater root progression and associated complications, usually take place in a more favorable biological setting than when the case is followed for a long time until it becomes symptomatic and more complex.
A 2024 study in the Journal of Oral and Maxillofacial Surgery showed differences in the reasons for extraction and in postoperative complications according to age, indicating that older patients tend to present removals associated with more advanced pathological conditions and greater clinical complexity.
This does not mean that “every wisdom tooth should be removed early.” It means something more refined: when there are signs that a third molar has a high potential to cause damage, waiting too long can negatively change the treatment scenario. And when the decision is to monitor, that monitoring needs to be real, planned, and documented.
Developing roots and a more predictable surgery
In many cases, one of the factors that makes surgery more favorable is the stage of root development. When the roots are not yet fully formed, removal may be less traumatic from a technical point of view compared with cases in which they are already fully developed, possibly curved, or in close relation to the inferior alveolar nerve. This reasoning appears frequently in the literature on third molar management and also in the practice of oral and maxillofacial surgeons.
Of course, this is not an absolute rule. There are cases in which, even with partially formed roots, the best course is monitoring. And there are cases with fully developed roots in which extraction remains the best decision. The point is that tooth biology and developmental stage make a real difference in surgical strategy, operative difficulty, and certain specific risks.
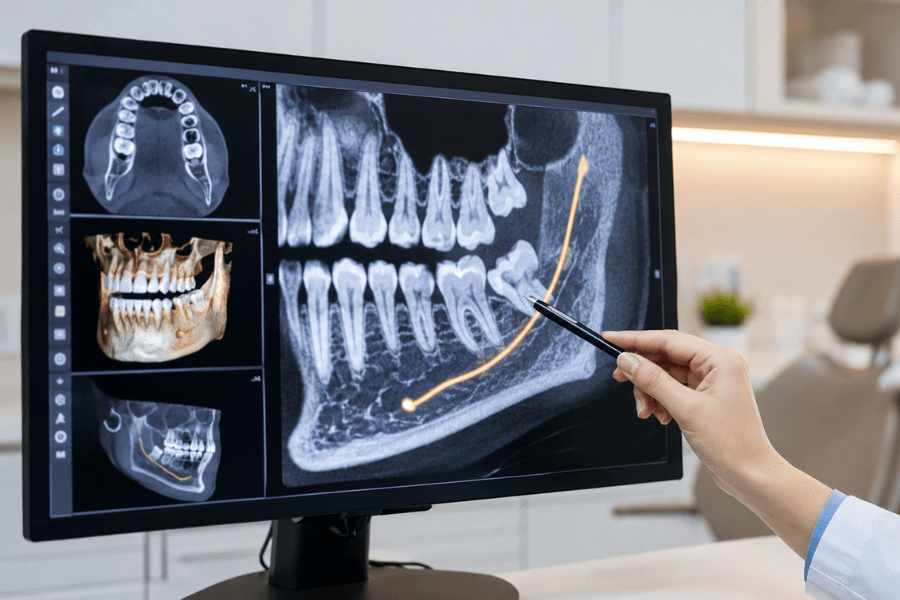
Where does the 3D exam come in?
When we talk about a 3D exam for wisdom teeth, we are usually referring to cone beam computed tomography, or CBCT. This exam is not necessary for every patient, but it has become extremely valuable in cases where it is necessary to precisely understand the position of the tooth, the morphology of the roots, the depth of impaction, and especially the relationship of the lower wisdom tooth with the inferior alveolar nerve. Recent reviews show that CBCT offers superior three-dimensional visualization compared with panoramic radiography for this type of risk analysis.
In practice, this changes decision-making. With a well-indicated 3D evaluation, it is possible to determine whether the case calls for immediate extraction, whether it is worth discussing alternatives such as coronectomy in specific situations of high neural risk, or whether the best path is monitoring. The value of the exam is not in “requesting technology for its own sake,” but in obtaining the right information to protect the patient and plan the surgery with greater precision. AAOMS itself highlights the role of advanced imaging in evaluating third molars close to the nerve and in defining the surgical plan.
When the pain comes late, the case may already be more complex
Many patients seek help only when wisdom tooth pain becomes undeniable. At that stage, it is not uncommon to find inflamed tissue, recurrent infections, compromised hygiene in the region, damage to the neighboring tooth, and roots that are already fully formed. In addition, the surgery may require greater osteotomy, more odontosection, and even more careful planning to reduce the risk of trauma to the nerve, bone, and soft tissues.
This is not about creating fear, but about communicating the difference between a problem identified early and one treated only after it has moved beyond the initial stage. Excellent dentistry works precisely to reduce this delay. When evaluation happens at the right time, the decision can often be made in a more favorable scenario, with greater predictability for both the patient and the team.
Extraction is not the only answer
It is also important to say clearly: not every wisdom tooth with mild discomfort needs to be removed immediately. Evidence-based guidelines recommend that the indication for extraction be supported by clinical signs, imaging, risk of progression, and the real possibility of monitoring. When there is no disease in place and no signs of imminent damage, follow-up may be a valid approach, as long as it is organized and not simply “wait and see later.”
At Clínica Debora Ayala, this point is central. The patient’s peace of mind does not come from a rushed decision, but from the certainty that there is a strategy. If extraction is the best course, it should be performed at the moment that offers the greatest safety and predictability. If monitoring is the best conduct, it must be done with proper clinical examination, imaging, and follow-up to prevent the problem from progressing silently.
What characterizes excellent care in this area
Speaking of excellent care for wisdom teeth means abandoning the simplistic logic of “wait until it hurts a lot” or “remove them all right away.” What defines excellence is the combination of listening, detailed clinical examination, well-indicated imaging, and personalized decision-making. It means understanding that patient’s anatomy, the stage of tooth formation, the type of impaction, the current symptoms, the future risks, and the biological reality of the case.
That is why wisdom tooth evaluation must be treated seriously. Mild discomfort at the back of the mouth may indeed be the first sign that something needs attention. But the best result does not depend only on recognizing the symptom. It depends on acting at the right time, with the right diagnosis, and with the right strategy.
Take care of wisdom tooth pain with precision and safety
If you feel wisdom tooth pain, pressure at the back of the mouth, discomfort while chewing, or notice that the posterior region is more sensitive and harder to keep clean, this is the time to investigate. The pain may be subtle today, but what really matters is understanding what it is signaling and what the best course of action is to preserve your oral health safely.
At Clínica Debora Ayala, third molars are evaluated with a meticulous clinical examination and, when indicated, with a 3D exam, in order to define whether the best strategy is extraction at the ideal moment or responsible monitoring. The goal is not to rush surgery without criteria or to delay an important decision. It is to offer you the most precise, predictable, and safe course of action.
Get in touch and schedule your personalized consultation with Dr. Debora Ayala. Together, we will define, with technical rigor and clinical insight, the strategy that best protects your smile and your oral health.
Dr. Debora Ayala – CRO 41.974/SP
Sources:
Sánchez-Garcés, M. Á. et al. Diagnosis and indications for the extraction of third molars: Clinical Practice Guideline. PMC. Disponível em: https://pmc.ncbi.nlm.nih.gov/articles/PMC11249379/. Acesso em: 12 maio 2026.
Sun, R. et al. Expert consensus on the management of third molar health. PMC. Disponível em: https://pmc.ncbi.nlm.nih.gov/articles/PMC13079848/. Acesso em: 12 maio 2026.
American Association of Oral and Maxillofacial Surgeons. White Paper on Third Molar Data. Disponível em: https://aaoms.org/wp-content/uploads/2024/03/white_paper_third_molar_data.pdf. Acesso em: 12 maio 2026.
American Association of Oral and Maxillofacial Surgeons. Evidence-Based Management of Third Molar Teeth. Disponível em: https://aaoms.org/wp-content/uploads/2022/06/evidence_based_management_third_molars.pdf. Acesso em: 12 maio 2026.
Di Spirito, F. et al. Impacted Mandibular Third Molar: Approaches and Current Perspectives. PMC. Disponível em: https://pmc.ncbi.nlm.nih.gov/articles/PMC12472061/. Acesso em: 12 maio 2026.
Kim, J. Y. et al. Are There Differences in the Causes and Complications of Impacted Third Molar Extraction According to Age? Journal of Oral and Maxillofacial Surgery / ScienceDirect. Disponível em: https://www.sciencedirect.com/science/article/abs/pii/S0278239124005925. Acesso em: 12 maio 2026.
Shokri, A. et al. Radiographic relationship of third molars with the mandibular canal: panoramic imaging versus CBCT. PMC. Disponível em: https://pmc.ncbi.nlm.nih.gov/articles/PMC12210119/. Acesso em: 12 maio 2026.
Dignam, P. et al. Prevalence and Factors Influencing Post-Operative Complications Following Third Molar Surgery. PMC. Disponível em: https://pmc.ncbi.nlm.nih.gov/articles/PMC11098612/. Acesso em: 12 maio 2026.
Read Also
